Multiple Sclerosis - A Common Virus May Result In New Therapies
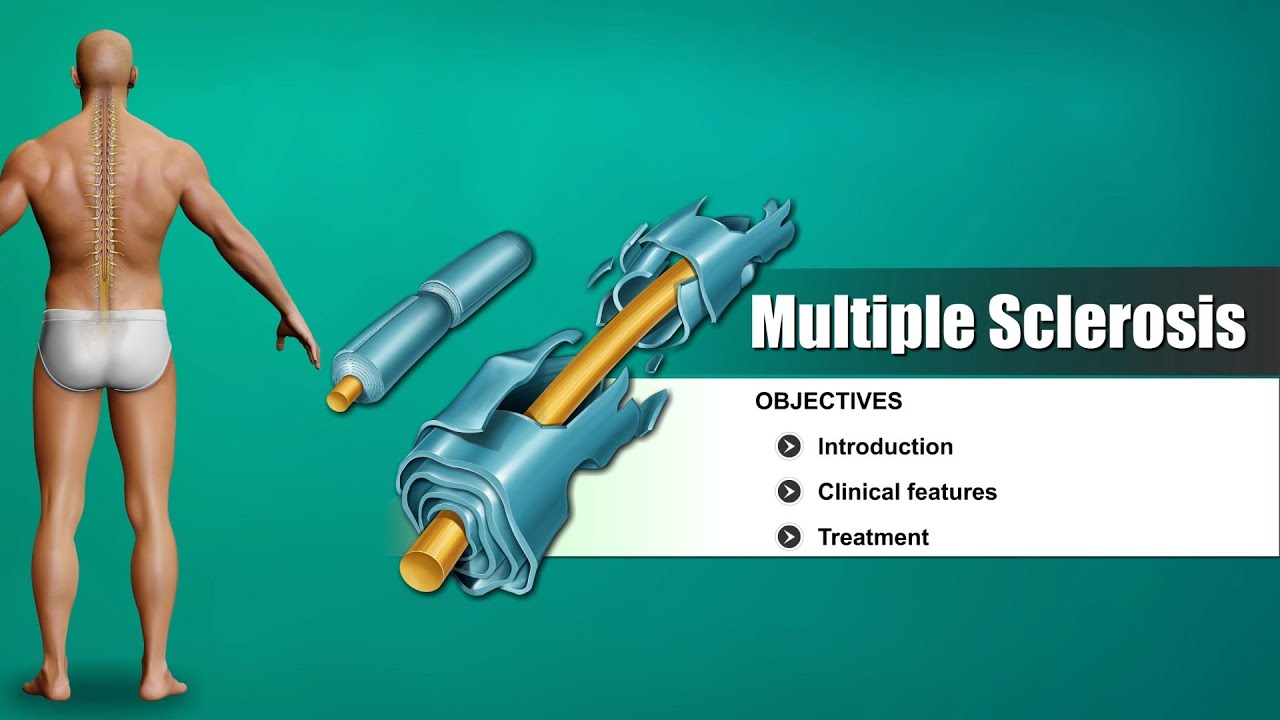
Most doctors agree that multiple sclerosis (MS) is an autoimmune disease where the body's immune system attacks healthy tissues by accident. The myelin sheath, which typically shields nerve fibers in the central nervous system, is attacked in MS by the immune system. In this attack, the underlying nerve fibers may also be harmed or killed.
Author:Stefano MclaughlinReviewer:Dexter CookeMay 30, 202343.2K Shares1M Views

Most doctors agree that multiple sclerosis(MS) is an autoimmune disease where the body's immune system attacks healthy tissues by accident.
The myelin sheath, which typically shields nerve fibers in the central nervous system, is attacked in MS by the immune system.
In this attack, the underlying nerve fibers may also be harmed or killed.
Symptoms are caused by areas of sclerosis that block electrical signals between the brain and other parts of the body.
This happens when the myelin sheath becomes irritated and gradually damaged as the attack continues.
Some scientists disagree with the autoimmune theory of multiple sclerosis.
Some people have said that the damage to the nerve fibers is caused by another disease process and that the inflammation caused by MS is just a reaction to the damage, not the cause.
Better imaging technology and more research are needed to learn more about what causes MS and which treatments work best.
What Is Multiple Sclerosis?
Multiple sclerosis is a type of autoimmune disorder.
When you have these disorders, your immune system incorrectly assaults healthy cells.
The immune system targets cells in the myelin, the protective sheath that covers nerves in the brain and spinal cord in people with MS.
Damage to the myelin sheath causes nerve transmissions from your brain to other parts of your body to be disrupted. The injury may cause symptoms in your brain, spinal cord, and eyes.
Multiple sclerosis is classified into 4 types:
Clinically Isolated Syndrome (CIS)
When someone experiences their first episode of MS symptoms, healthcare providers frequently classify it as CIS.
Not every person with CIS develops multiple sclerosis.
Relapsing-Remitting MS (RRMS)
This is how the vast majority of MS cases manifest.
Flare-ups, also known as relapses or exacerbations, are periods of new or worsened symptoms experienced by people with RRMS.
Next, there are lulls in the action.
Primary Progressive MS (PPMS)
In people with PPMS, the decline in function is progressive and uninterruptible by remission.
Secondary Progressive MS (SPMS)
Those who were first diagnosed with RRMS often develop SPMS as time goes on.
You have a kind of MS called secondary progressive if you're always suffering from new nerve damage.
You're seeing a steady escalation in your symptoms' severity.
After that, you won't have any more remission periods.
Instead, you'll have relapses or flares, which are times when your symptoms get worse.
Mayo Clinic Explains Multiple Sclerosis
What Causes Multiple Sclerosis?
Experts are still unsure about the precise cause of multiple sclerosis. Research is ongoing to assist in pinpointing the disease's underlying causes. Several things can cause MS, such as:
Exposure to certain viruses or bacteria
Some studies show that a person may get MS later in life if they are exposed to certain illnesses like the Epstein-Barr virus.
Your environment
Your chance of getting MS may be influenced by your environment.
The prevalence of the disease is noticeably higher in some regions of the world than in others.
MS is more prevalent in regions that are farthest from the equator.
That might be because the sun doesn't shine as brightly in certain areas. A risk factor for MS development is reduced vitamin D levels in people who spend less time in the sun.
How your immune system functions
Multiple sclerosis is an autoimmune disease, which affects the way your immune system works.
Researchers are trying to determine why immune cells in some people attack healthy cells inadvertently.
Gene mutations
Having an MS-afflicted family member does enhance your likelihood of developing the condition.
But scientists still don't know exactly how and which genes cause multiple sclerosis.
A Familiar Virus
About 3 million people around the world suffer from multiple sclerosis, making it a relatively rare disease. However, the Epstein-Barr virus is ubiquitous.
Since its discovery in 1964, the virus has spread throughout the world, infecting an estimated 90% of the population.
Those who were infected as kids might only develop a mild cold or show no symptoms at all.
Infectious mononucleosis can cause severe fatigue in teenagers and young adults that can last for weeks or months.
Eventually, these effects will disappear.
Epstein-Barr virus infections persist, however.
The virus is related to other herpes viruses, which are notorious for causing chronic infections.
The herpes viruses that cause cold sores, genital herpes, and chickenpox are also persistent, although they often do not manifest for years at a time.
For example, the varicella-zoster virus, which causes chickenpox, can hide in nerve cells and wait for the right time to cause shingles, a very painful disease.
Because Epstein-Barr virus enters the epithelial cells that line the surface of the throat, mononucleosis is commonly referred to as "the kissing disease" because it is spread primarily through saliva.
The virus also gets into B cells, which are part of the immune system. Once inside B cells, the virus goes into a dormant state.
Establishing The Link
Studying the possible connection between Epstein-Barr virus and multiple sclerosis, Harvard T.H.
Chan School of Public Health epidemiology professor Alberto Ascherio presented his findings in March of 2000. Ascherio studied data from eight studies with her colleague Mette Munch of the University of Aarhus in Denmark and found that MS patients were more likely to have had an Epstein-Barr virus than those without MS.
Through the following two decades of research, hints that the virus is involved persisted, but "the challenge is to go from a suggestion or suspicion to proof," as Ascherio puts it.
Almost everyone has the Epstein-Barr virus (EBV), but only a small number of people get multiple sclerosis. This makes it hard to find evidence of this.
If "EBV causes MS," Ascherio says, "you would expect to find that those people who are not infected with EBV will not have MS." "It's a breeze," they said. He and his team had to keep tabs on a sizable population of adults in their 20s who had never been infected.
The researchers identified this subset within the American armed forces.
When active-duty personnel were examined for diseases like HIV at the beginning of their service and again every two years, the team had access to repeated blood samples from more than 10 million individuals through the Department of Defense Serum Repository.
By looking at blood samples taken between 1993 and 2013, Ascherio and his colleagues were able to find out when MS symptoms first showed up in people who had never been infected with Epstein-Barr virus.
Multiple sclerosis - causes, symptoms, diagnosis, treatment, pathology
A Skeptic Is Convinced
Tobias Lanz, a neurologist at Stanford University, said that many experts were skeptical of the relationship between Epstein-Barr virus and MS because the virus has been linked to so many other disorders.
It plays a role in cancer, multiple sclerosis, lupus, and chronic tiredness. People seem to connect it with everything, and that makes us very wary.
William Robinson, a rheumatologist and Lanz's mentor at Stanford, was a skeptic. Robinson was at first skeptical, but after Lanz and his team found proof that the Epstein-Barr virus can damage nerves, he changed his mind.
An important Epstein-Barr virus protein and a central nervous system protein were both shown to be bound by antibodies from MS patients.
The study says that as the immune system learns to recognize the virus, it may be taught to attack nerve cells.
Epstein-Barr virus, thanks in large part to a viral protein called EBNA1, may live indefinitely in the body where it hides away safely within B cells.
Experiments showed that the virus's antibodies also detect and bind strongly to its molecular twin, a piece of a protein called GlialCAM, in the central nervous system.
As Robinson puts it, this is "an in-your-face discovery that you can't ignore as not being real."
This result not only adds to the mounting body of evidence indicating the Epstein-Barr virus is responsible for multiple sclerosis, but it also suggests a potential mechanism; supportive glial cells called glial cells express glial cell adhesion molecule (glialCAM), which helps to insulate nerve fibers (myelin) and prevents electrical impulses (neurites) from leaking out.
The destruction of myelin is at the heart of multiple sclerosis.
Damage Of The Virus
Multiple sclerosis damage is caused by molecular mimicry, according to several studies. Of course, we can also consider alternative explanations.
Antibodies, for example, are made by the B cells where Epstein-Barr viruses like to lurk. An infection with the Epstein-Barr virus has been linked to a change in B cells that may cause the immune system to attack healthy tissue.
The body's immune response to the infection itself, says Roman neurosurgeon Aloisi, is another possible explanation. Aloisi explains that the virus and disease have "remarkably comparable biochemistry."
For some people with multiple sclerosis, the symptoms may seem to go away or at least stay the same.
Once active, the disease causes additional brain lesions and more severe symptoms. Like HIV, the Epstein-Barr virus can come out of hiding and spread before going back to hiding in the cells of its host.
Clusters of B lymphocytes were found in the membranes that surround and protect the brain, an unexpected discovery made by Aloisi and colleagues in 2007. Some of the B cells were infected with the Epstein-Barr virus in 21 of the 22 patients analyzed.
According to Aloisi, the discovery was "like a bomb in the field" because "nobody ever dreamed about this possibility."
Initial attempts by other researchers to duplicate the results were unsuccessful.
However, "little by little, other work came out," she explains. People with MS don't have very large or inflamed brains, which makes it harder to locate these clusters of B cells as it only appears in isolated locations.
Treatment Tactics
The matter at hand is treatment, not whether the Epstein-Barr virus actually causes MS symptoms or whether it triggers an autoimmune response gone awry.
Aloisi suggests developing antiviral medications for multiple sclerosis as a potential solution.
According to Ascherio, a Harvard epidemiologist, some medications that inhibit hepatitis B virus and HIV have shown promise against Epstein-Barr virus in laboratory-grown cells.
These findings, however, are still in the early stages.
Attacking the contaminated cells is another strategy. Maybe certain MS treatments are already doing that.
The current treatment for MS, natalizumab, already blocks B and T cells from entering the brain and spinal cord. That also might be achieved by fingolimod.
Ocrelizumab is an antibody that binds to a protein on B cells, leading to cell death and approval for use in MS patients in 2017.
People with relapsing-remitting MS, like Agosto, see more improvement from the medicine than people with the more progressive form of the disease, who have fewer treatment options.
Lanz explains that scientists believed the medication reduced inappropriate immune responses by eliminating B cells.
However, it is also possible that we are attacking pathogenic B cells that are infected with the Epstein-Barr virus.
B cell depletion might be a good way to treat EBV, but no one knew that at the time.
In this, Aloisi is in agreement. We need a treatment that "specifically targets the EBV-infected cells rather than the B cells as a whole," she says.
Taking out B cells without thinking can leave people vulnerable to additional illnesses. Perhaps T cell treatments that selectively target infected cells may be one solution to this problem.
Multiple sclerosis patients are already participating in clinical studies of such treatments.

A Vaccine
Preventing the spread of the virus in the first place, or even keeping it dormant, would be preferable to trying to stop an already-established illness from spreading. This led to the introduction of vaccines.
Several possible vaccines are already under development due to the extensive impact of mononucleosis and Epstein-Barr viruses' ties to cancer and autoimmune illness.
But Javier Gordon Ogembo, a vaccinologist at the City of Hope cancer care center in Duarte, California, says that the Epstein-Barr virus gets into the body in a complicated way.
Epithelial cells and B cells are invaded using at least five different viral proteins. In order to prevent infection, a vaccine would need to stimulate an immune response that prevents the virus from entering both types of cells.
This, according to Ogembo, is why there is no vaccination yet.
In the early 2000s, GlaxoSmithKline, a pharmaceutical corporation, sent a potential vaccine candidate into clinical trials.
Although it appeared to protect people from becoming mononucleosis, it fell short of the primary objective of preventing infection. The vaccination was therefore abandoned by the corporation.
Biotech powerhouse Moderna, best known for its very efficient COVID-19 vaccine, has just begun testing an mRNA vaccine against Epstein-Barr virus in humans.
According to viral immunologist Katherine Luzuriaga of the University of Massachusetts Chan Medical Center in Worcester, who is involved in the experiment, the shot teaches the body to detect four of the five viral proteins that let the virus infect both cell types.
The team is currently conducting tests to determine if the vaccination produces a significant immune response and if it has the potential to reduce mononucleosis outbreaks.
Clinical testing of a vaccine that uses nanoparticles to train the body to recognize and eliminate the virus began in March at the United States National Institutes of Health.
Ogembo and his team at City of Hope are working on a new vaccine.
People Also Ask
What Is The Main Cause Of Multiple Sclerosis?
We don't know what sets off MS attacks. It is considered an autoimmune disorder in which the immune system mistakenly assaults healthy tissue.
The immune system dysfunction that causes multiple sclerosis damages these fibers by attacking the fatty substance that coats and protects brain and spinal cord nerve fibers.
At What Age Does Multiple Sclerosis Usually Start?
People with multiple sclerosis (MS) tend to have their first symptoms between the ages of 20 and 40. Usually the symptoms get better, but then they come back.
Some come and go, while others linger. No two people have exactly the same symptoms.
How Serious Is Multiple Sclerosis?
There is usually no way to prevent multiple sclerosis from shortening your life by a few months. Most anxiety about a prognosis is about the quality of life and the chance of being disabled.
How Do They Test For Multiple Sclerosis?
Magnetic resonance imaging (MRI) scans, taken after preliminary blood testing, are the gold standard for diagnosing multiple sclerosis.
Magnetic resonance imaging (MRI) machines employ radio waves and magnetic fields to measure how much water there is in a patient's tissues.
They have the ability to recognize abnormalities and distinguish between healthy and diseased tissues.
Conclusion
Even though they may get tired easily and may struggle to keep up with a demanding schedule, people with multiple sclerosis can frequently maintain an active lifestyle. Reassurance and encouragement are helpful.
Regular exercise, such as walking, swimming, stationary cycling, or stretching, lessens spasticity and promotes cardiovascular, musculoskeletal, and mental health.
Physical therapy can aid in preserving mobility, range of motion, and balance and can lessen stiffness and weakness.
Walking alone should be encouraged for as long as possible. By doing this, their quality of life is enhanced and depression is prevented.
Doctors typically advise patients to take vitamin D supplements because low vitamin D levels are associated with more severe multiple sclerosis and because supplementing with vitamin D may lower the risk of osteoporosis.
Vitamin D pills are being looked into to see if they can slow down the progress of multiple sclerosis.

Stefano Mclaughlin
Author
Stefano Mclaughlin is a Psychologist focused on mental health, emotional well-being, and healthcare policy. He studied Psychology and Public Health at the University of Massachusetts Amherst, gaining a deep understanding of the intersection between mental health and public policy.
Stefano's mission is clear: he aims to destigmatize mental health discussions, improve access to mental healthcare, and promote emotional well-being for all. Drawing from personal experiences with anxiety and depression, Stefano shares real stories to make mental health topics more relatable and less intimidating.
In addition to his advocacy work, Stefano enjoys delving into books, experimenting in the kitchen, and embarking on new adventures. These hobbies fuel his creativity and inspire fresh perspectives for his advocacy work.

Dexter Cooke
Reviewer
Dexter Cooke is an economist, marketing strategist, and orthopedic surgeon with over 20 years of experience crafting compelling narratives that resonate worldwide.
He holds a Journalism degree from Columbia University, an Economics background from Yale University, and a medical degree with a postdoctoral fellowship in orthopedic medicine from the Medical University of South Carolina.
Dexter’s insights into media, economics, and marketing shine through his prolific contributions to respected publications and advisory roles for influential organizations.
As an orthopedic surgeon specializing in minimally invasive knee replacement surgery and laparoscopic procedures, Dexter prioritizes patient care above all.
Outside his professional pursuits, Dexter enjoys collecting vintage watches, studying ancient civilizations, learning about astronomy, and participating in charity runs.
Latest Articles
Popular Articles